Veterans Administration Secretary Denis McDonough visited Sioux Falls last week to talk about staffing issues at the Sioux Falls VA hospital and the major changes the VA is recommending to facilities and services nationwide. In March the VA issued recommendations that include scaling back some services in Sioux Falls in favor of partnerships with the private sector and, more dramatically, replacing the Fort Meade and Hot Springs hospitals with one new VA hospital in Rapid City. Secretary McDonough says those changes are part of a nationwide effort to provide better access to care at lower costs:
The bottom line is that all the recommended changes—if approved—will add up to the one thing that matters most: more care, and better care, for Veterans. If we implement these recommendations, for example, nearly 150,000 more Veterans will have primary care within 30 minutes; nearly 200,000 more Veterans will have mental health care within 30 minutes; and over 375,000 more Veterans will have access to outpatient specialty care within 60 minutes. In summary, all of that care will be delivered in modern, state-of-the-art facilities that Veterans deserve and will result in more Veterans’ lives saved, and improved, by the work VA does—which is precisely what these recommendations strive to accomplish [Secretary Denis McDonough, Department of Veterans Affairs, Foreword, VA Recommendations to the Asset and Infrastructure Review Commission, Vol. I, p. iii].
The median age of VA facilities is nearly 60 years old, compared to a median age of 8.5 years for U.S. private sector hospitals. In addition, 69% of VA hospitals are over 50 years old [VA Recommendations, Vol. I, March 2022, p. v]. All three South Dakota VA hosptials exceed the median age: the Sioux Falls hospital was built in 1948; Fort Meade, 1958; Hot Springs, 1926. Those old hospitals require a lot of upkeep.
Enrollees and eligible veterans will decline nationwide. Compared to Fiscal Year 2019, enrollees will drop 1.3% by FY2029 and 8.3% by FY2039. Eligible veterans will drop 14.8% by FY2029 and 26.9% by FY2039 [Vol. I, p. 14].
But enrollee populations won’t go down everywhere. Veterans are moving south and west, but facilities built 50 years ago aren’t moving with them.

Compounding the difficulty in providing efficient care is the rural inclinations of veterans. 33% of VA enrollees live in rural areas, higher than the 19% of the general population that lives in rural areas. Rural veterans are also more likely to enroll—58% of rural veterans enroll, versus 37% of urban veterans—likely because the private sector provides fewer healthcare options in rural areas. More veterans may choose to live in rural areas, but doctors and nurses don’t, so the VA has to compete with the same market factors that draw health care professionals to higher-pay, higher-opportunity urban markets to keep services within reach for its rural enrollees. The VA Recommendations include higher pay, new incentives and bonuses, and expanded student loan repayment, so saving money on facilities will help pay for staff.
Declining populations don’t mean less demand for all services. While demand for most inpatient services will decrease over the next ten years, demand for outpatient services will increase:
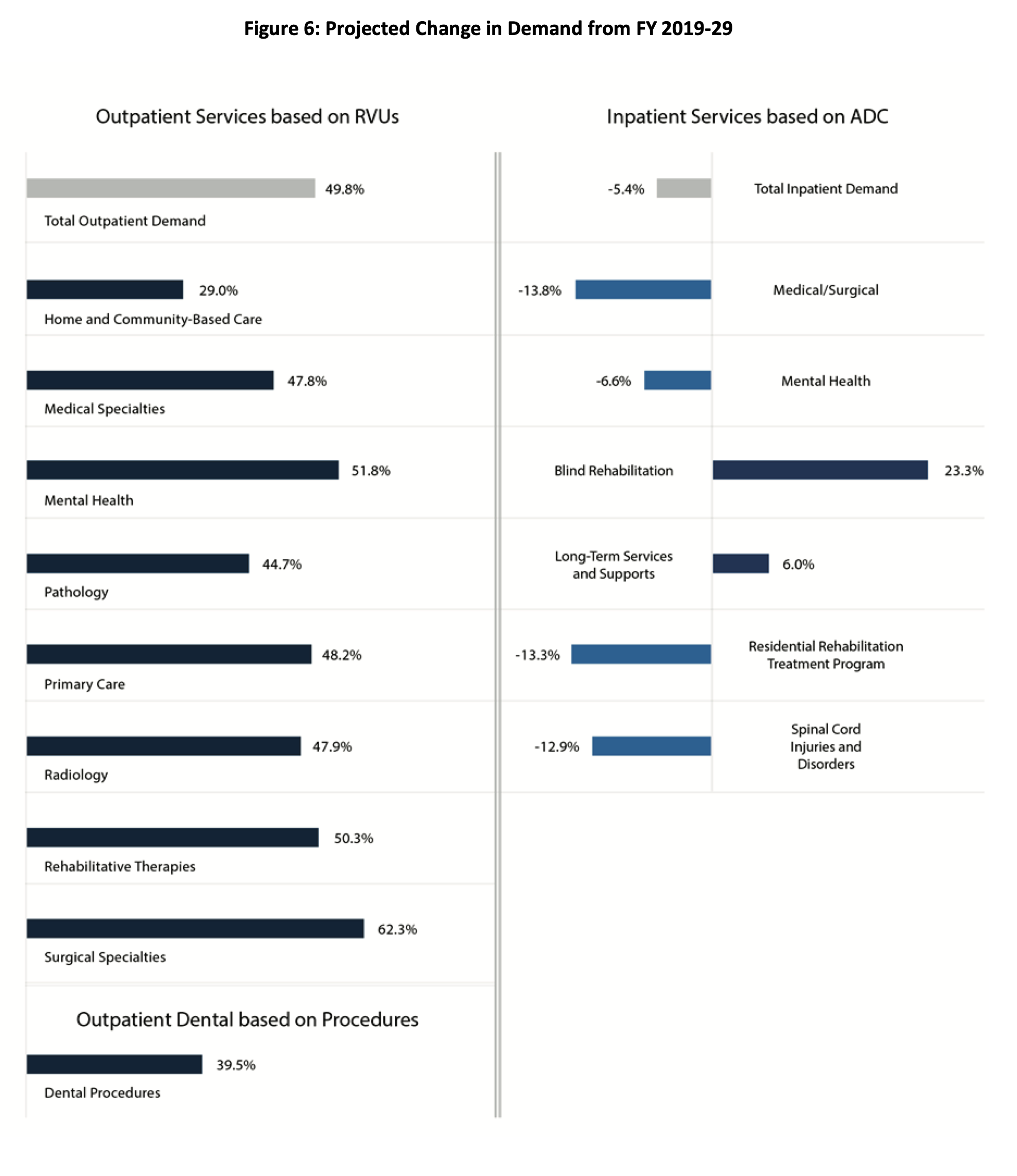
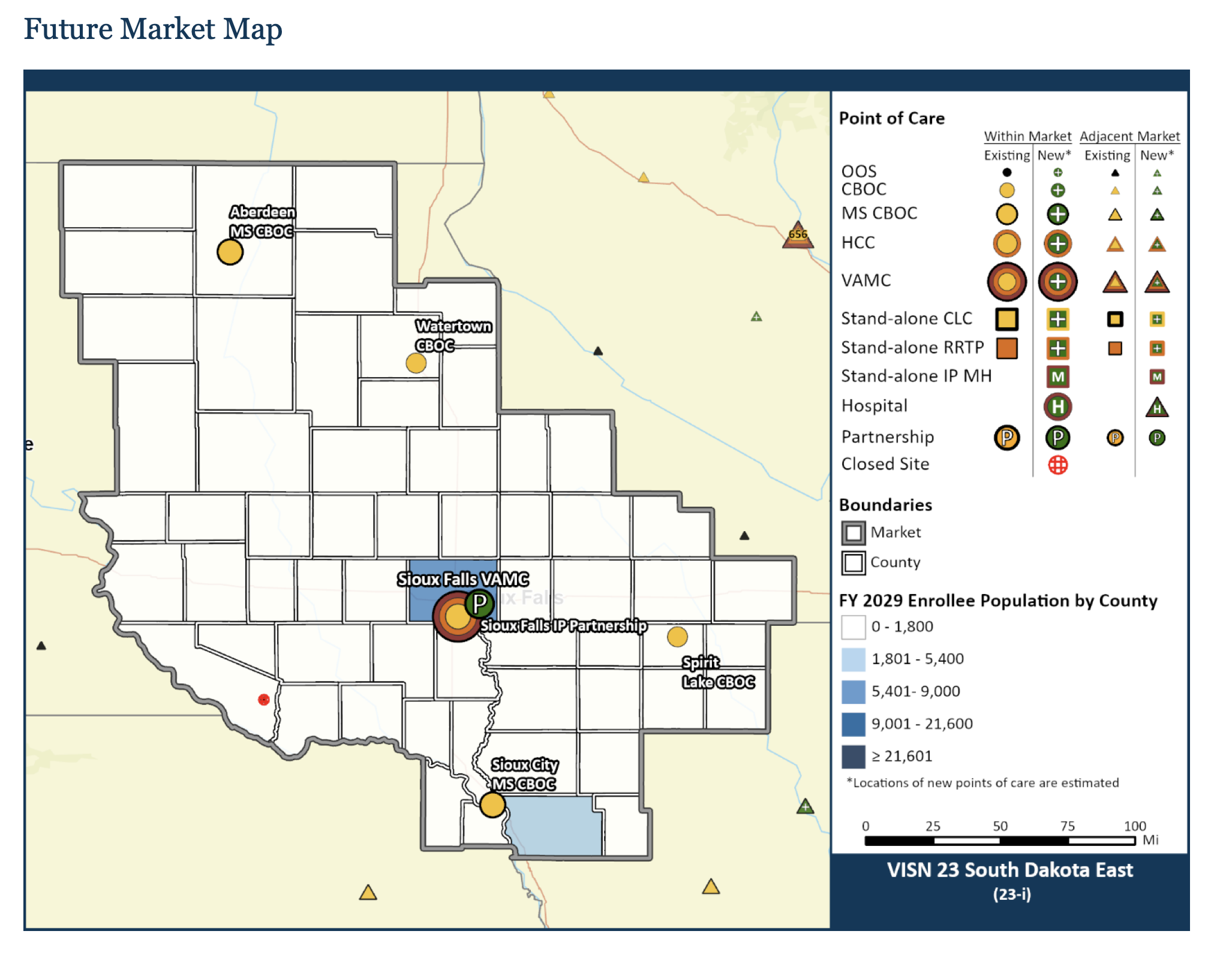
The VA divides South Dakota into two markets, East and West. East includes most of East River east of the 100th Meridian, minus Roberts County (considered part of the North Dakota market), plus southwestern Minnesota, northwestern Iowa, and the two Nebraska counties across the river from Sioux City and Vermillion. Enrollees in SD East will decrease 11.7%, a notably larger drop than the national decrease of 1.3%, from 33,611 in FY2019 to 29,700 in FY2029, yet demand will increase for all service categories: inpatient medical and surgical services up 7.6%, inpatient mental health services 8.9%, and long-term care 21.5%. Demand for outpatient services will increase.
The VA recommends increasing community living center beds from 58 to 88 at the Sioux Falls VA hospital, turning the emergency department into an urgent care center (as usage is 38% below the minimum VA recommends for maintaining emergency services), and shifting inpatient medical and surgical services to a partnership or community providers, who, according to the VA, are operating at only 53.6% capacity and can easily absorb VA demand. The VA recommends closing the Wagner outpatient clinic and shifting those patients to the Wagner IHS clinic and community providers in Mitchell or Yankton.
These major changes and a raft of complementary proposals would cost 1.6% more than doing nothing different. But modernizing existing facilities to maintain all current services and facilities would cost 6.6% more than the current system. The recommended changes involve increased capital spending up front but lower operational costs by 5.1%.
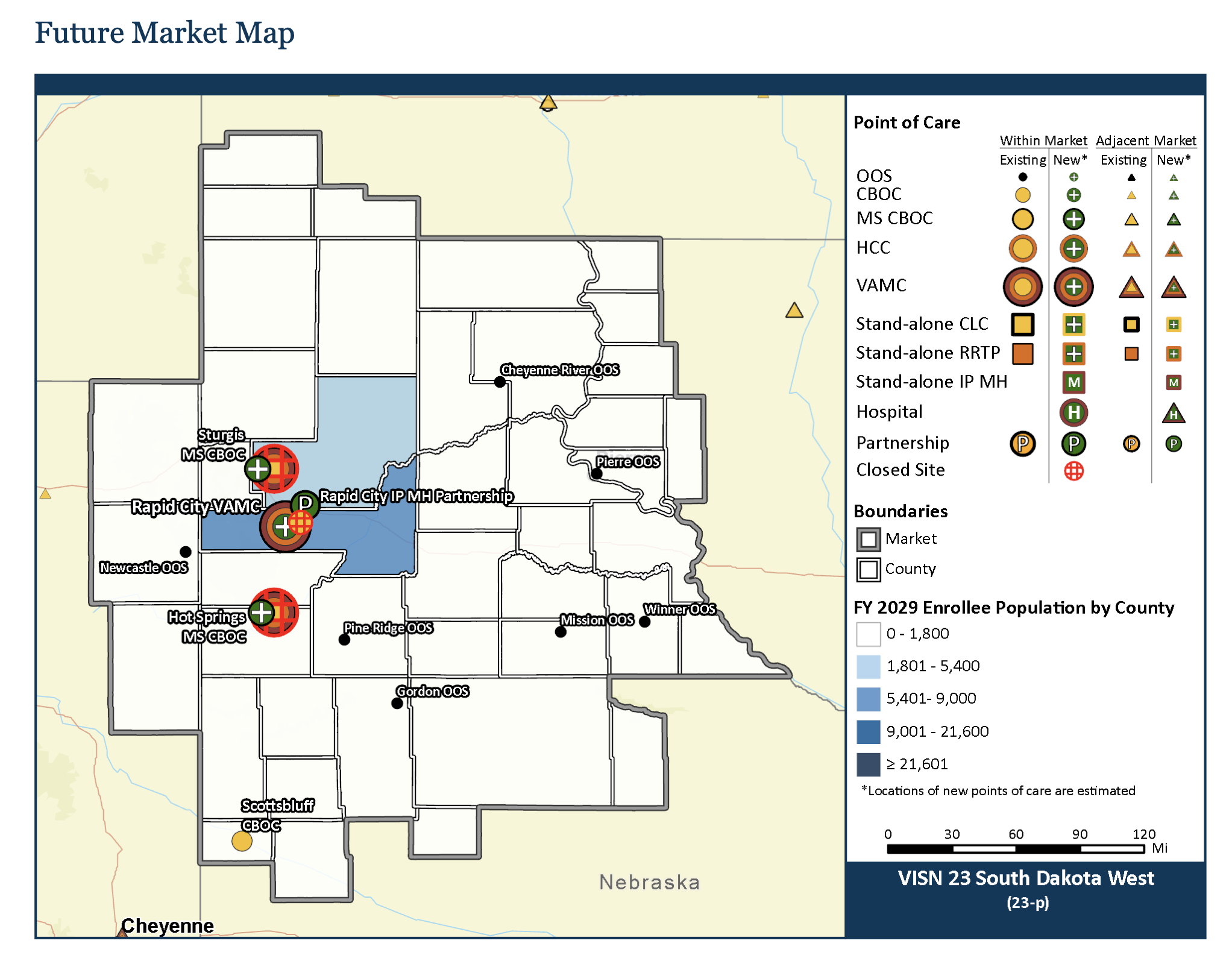
The South Dakota West market is all of West River plus Pierre, Highmore, and Mobridge, plus northeastern Wyoming, northwestern Nebraska, and a bit of southwestern North Dakota. Enrollees in SD West will decrease 6.8% by FY2029, from 21,332 to 19,900. Demand for inpatient medical and surgical care will decrease by 9.8%, and demand for mental health services will decrease 13.2%. Demand for long-term care will increase 6.9%. Demand for outpatient services will increase.
SD West has two-thirds as many enrollees as SD East, yet it has two full VA hospitals, in Fort Meade and Hot Springs, while SD East has one, in Sioux Falls. The VA contends two full facilities in SD West are unsustainable. The VA thus proposes building one new VA hospital in Rapid City with 46 rehab beds and 54 community living center beds. The VA would move outpatient services from its current Rapid City outpatient clinic to the new hospital and close the clinic, which lacks space to expand. The VA would shut down the Fort Meade and Hot Springs hospitals and build one new outpatient clinic in Sturgis and one in Hot Springs. The VA recommends maintaining the other eight outpatient facilities around the SD West market.
Combined with other proposed changes, building a whole new hospital in Rapid City and closing the Fort Meade and Hot Springs hospitals would cost 4.8% less than making no changes and 5.2% less than the modernization that the current facilities across SD West require. The recommended changes lower capital costs by more than 3% and lower operational costs by 5.0%.
- AIR Commission reports to President by Jan. 31, 2023.
- President approves/disapproves by Feb. 15, 2023.
- President must submit to Congress by March 30 or process ends.
- Congress has 45 days to disapprove; otherwise, recommendations implemented by Feb. 15, 2026.
The VA says it can provide more enrollees easier access to quality health care with this plan. South Dakota East requires upgrades to its central hospital but no relocation, since Sioux Falls is the most central location for the market and the best place to recruit doctors and nurses. We may worry that closing the Fort Meade and Hot Springs hospitals will cause job loss, but the way the workforce is trending, we’re not going to be able to hire enough doctors and nurses and other workers to fully staff those facilities. Centralizing inpatient services in Rapid City puts those services in easier reach of more veterans and it puts the work site in the one much larger community where the spouses of those health care workers would probably be looking for jobs anyway.
Our political leaders have sounded the usual alarms, but they need to provide some hard evidence to counter the improvements in access and cost savings that the proposals offer for the VA.
The Republican government shutdown and the 2013 sequester not only ripped into military readiness, the impacts on personnel are staggering. Since the second Bush administration invaded Afghanistan and Iraq over 30,000 veterans have died by suicide compared to 7,057 who died from combat related injuries according to research conducted by the Watson Institute at Brown University.
There is a growing movement among Democrats and others to fund Medicare for all but I like the idea of rolling the funding for Obamacare, TRICARE, Medicare, the Indian Health Service and the VHA together then offering Medicaid for all by increasing the estate tax, raising taxes on tobacco and adopting a carbon tax.
I agree with consolidations with new facilities. I also agree with the consolidation of school districts and county seats. There is a strong need for dumping the old and embracing the new.
If the Sioux Falls VA is indicative of the VA standard of care generally, just privatize it. My care has been atrocious.
Dicta, there were veterans at the meeting with Secretary McDonough saying just the opposite, that they get the best care anywhere at the SF VA and don’t want the VA to privatize their care.
I have had to fight for refills on meds, battles with care in the community, referrals promised that never happened, meetings cancelled as I drove to them from hours away, etc. They may like it. I hate the VA right now. A lot.
Remember that the highest percentage of combat veterans and combat related disabilities come from rural areas….as the voice over in “Platoon” states “there are guys here from places you’ve never heard of.” Native Americans were placed in combat infantry regiments and served as medics at the highest percentage of any race in the service.
PRIORITY POPUATIONS DEFINED
The definition of priority populations is broad, including people of color; veterans; LGBTQ people; people who are homeless or in the criminal justice system; people who have HIV or AIDS; older adults; “children and families”; and people with disabilities.
The VA system will eventually/soon be reorganized to provide specialized care from specially trained staff to include all groups above and some that haven’t been recognized, yet.
There are veterans advocates at the facilities. If you’re a wounded veteran (mentally or physically), join the DAV for assistance in getting your rights fulfilled. The DAV helped both me and my son with several issues over the years, I recommend them strongly.
If you’re a veteran who has served, make sure to have all your documents like the DD214 in place and if you’re on Medicare, understand that the VA might not give you any better coverage than you presently get with your supplement. Even the right wing American Legion will offer help that may help your frustration. You can also access the VA’s website and get signed in for your needs.
Don’t count on EB5 Rounds, Russo Thune or Dirty Johnson for assistance. They will send you a fakey letter that says what a great job they’re doing screwing veterans. They may help you if you mention you like Putin, that seems to perk them up.
My VA care and my father’s VA care has been exceptional. I understand the efficiency of consolidation, be it counties or the VA, but city folks should understand, not everyone can move from their rural areas. When the US called,efficiency was not considered, and we stood up and served instead faking heel spurs or having other priorities. For some, being a recluse is a benefit to society.
I worked in a VA Medical Center for 25 years. The charts appear to be construed the same way as the prior recommended closing of Hot Springs when they left off parts of the catchment area They left eastern Montana off the catchment area in this case. Vets come to Ft Meade because it is closer than Ft Harrison.
The big savings are in support services. Both Hot Springs and Ft. Meade have their own Fire Departments (Local VFDs do not meet VA Response requirements), roads and grounds, water treatment (Ft Meade) plus maintaining numerous old buildings including out buildings such as quarters, shops and admin space. The new hospital in RC eliminates some of these services.
Some of the proposals require action by congress. I do not see any many changes for years.
Larry seems to have it down. The major part of the problem is dealing with the present and not what would be the best.
It would be interesting to know how Fischer, Rounds and Associates is weathering the costs of hospital stays and Covid payouts without help from the feds. There are loads of Republicans on the list.
https://www.siouxfalls.business/sba-releases-list-of-businesses-that-benefited-from-ppp-loans/
This simply ain’t gonna happen. There are not enough votes to even have a commission. My ado about natta. More drama before the midterm elections that our crooked congress critters will milk to the very end. A good Democrat or an Independent should get right on this and act like your fighting tooth and nail to keep things the way they presently are. Be louder than the current crooks and liars. Nothing is gonna change regarding closing existing hospitals, simply ain’t gonna happen.
“your” equals you’re