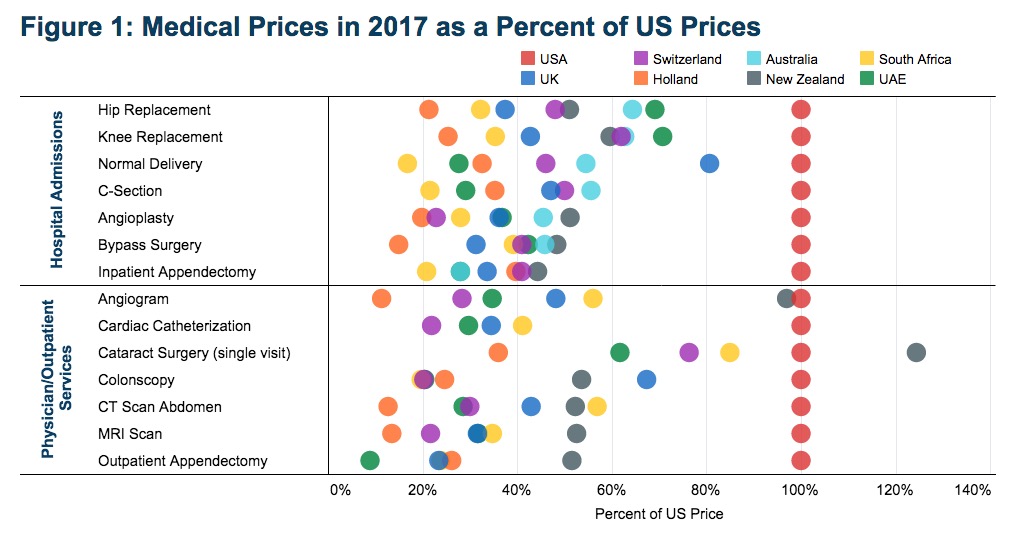
Naysayers who want to stick in the mud of America’s failing for-profit health care system say we can’t afford Medicare for All. But we’re already paying much more for basic medical procedures than nations that do something like Medicare for All.
So says the International Federation of Health Plans in its latest International Comparative Price Report. If you went to the hospital in 2017, you paid more for pretty much everything than you fellow patients in the United Kingdom, Switzerland, Holland, Australia, New Zealand, South Africa, and the United Arab Emirates, all of which do some form of universal health care:
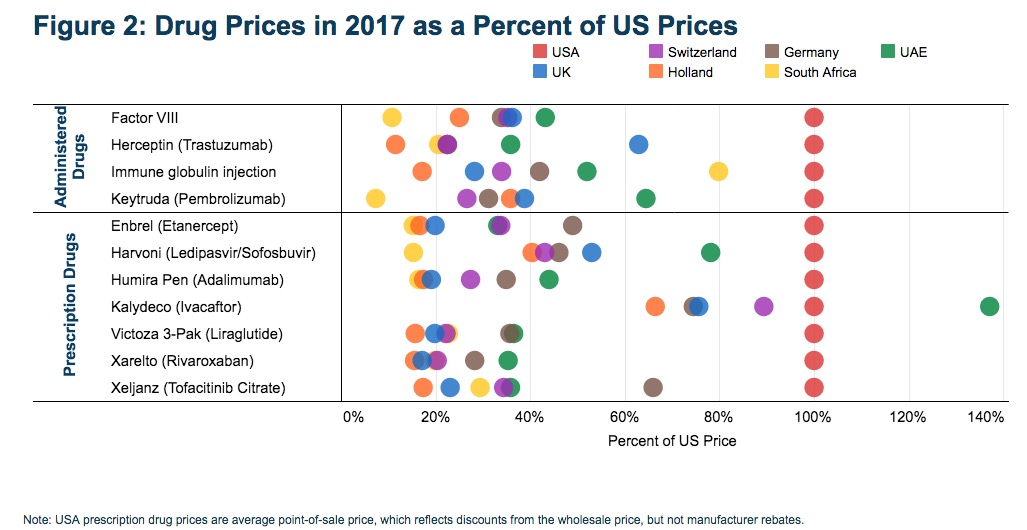
You also paid more for most of your drugs than our more sensibly socialist global counterparts:
As Senator Bernie Sanders reminds us, if we can afford these crazy costs, we can totally afford to follow the model of other nations and work together as a nation to cover everyone’s medical bills.
The obvious missing element of these studies are waiting times by patients seeking these procedures. Also, these charts don’t incorporate positive/negative outcomes of the procedures. How about the cost per citizen or the tax burden on each citizen to support this? Sure – on paper, these neat colorful dots represent cost differential, but without the entire picture – that all they are – dots on a graph. Does something need to be done to lower costs? Of course. Does the government need to run healthcare? Absolutely not.
Realist makes a good point – we really should look at studies about “waiting times” in countries with socialized medicine compared to the U.S. Here is some information I found in a quick look on the net:
One source reported that “waiting times” for immediate need medical appointments was longer in Canada compared to the U.S., but substantially shorter in several other countries with socialized medicine for “adults who made a same-day or next day appointment when needed care, 2016.” The percentage of people receiving quick care are reported to be:
Netherlands 77%
Australia 67%
United Kingdom 57%
France 56%
Germany 53%
United States 51%
Sweden 49%
Canada 43%
https://www.healthsystemtracker.org/indicator/access-affordability/4578-2/
Additional research reports more details about the Canadian experience:
http://www.pnhp.org/facts/myths_memes.pdf
These studies support a conclusion that “waiting time” is not caused by socialized medicine and hence not a valid objection to implementation of socialized medicine in the U.S.
Medicare costs $144.60 per month and prescription drugs cost $42.00 per month, automatically withdrawn before check is deposited in my account.
The gubmint keeps costs down by negotiating procedure prices they are willing to pay. Then medicare covers 80% of that amount and I am responsible for the other 20%.
I am thinking we really need government run healthcare.l I have had no problems getting appointments in a timely fashion.
Realist reels off the standard excuse for doing nothing. Ask someone in rural South Dakota how long the wait times are to see a local physician for a simple annual checkup, and it will be infinite, because there is no local physician. Of course, there is the benefit that by not getting a checkup that rural South Dakotan will not have to pay anything for medical care. Rationing by geography happens all over rural South Dakota, and results in a large “wait time by geography.”
Wait times for critical services, though, are about the same. If you have a heart attack, you are going straight to emergency, various tests will be performed and one or more procedures are going to be performed stat. Anything that threatens your life or could threaten your life is going to be treated quickly no matter where you live. Then you get the bill or more likely in the US several rounds of statements that make no sense, and sort of wish you had died.
There is another sort of “wait time” that Realist isn’t considering. Many folks don’t go to the doctor to deal with situations that later become an emergency, because they can’t afford the appointment or the treatment. “Wait times by way of unaffordable medical charges” are far, far bigger problem overall than times to wait for a doctor appointment or procedure.
I had to get a dog bite treated and go through the rabies series. To do that I went to urgent care as fast as I could. Do you think, as my hand was bleeding and I could see my tendon in the hand, that I was going to go rationally comparison shopping for the best price and service? But that’s what the free market theory assumes, and that’s why, Realist, the free market doesn’t work in a lot of health care.
My problem with Medicare For All is that it leaves the private sector too much in control. I want a national health system. That ain’t going to happen, and probably Medicare For All is not either. I’d be fine with an approach that makes step-wise improvements.
Bearcreekbat – yes, lets rely on late 1990s data and a website to fully negate the waiting times argument. Yet, as recent as 2017 the Canadian health care system reported a waiting time of 13.3 weeks for medically necessary procedures, such as an angioplasty (https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3633404) And Congress had a Canadian doctor testify recently that wait times are a valid concern.
As long as we consider corporations “people” and money “free speech,” I would guess that things will not get better. I’m pretty sure any drug company can afford more lobbyists than I.
Realist implies that the date of a study somehow weakens its impact. The problem with that argument, however, is that the “waiting time” contention is based on an alleged inherent problem with the system rather than than its implementation at any given time. And while there certainly can be problems with implementing a system such problems are certainly solvable.
As for Canada, I note that one problem with implentation seems to be a reported underfunding of the system. This indicates that an adequately funded system would be a huge step toward resolving any waiting period issues. Indeed that seemed to be the case with the countries listed in the above link that reported shorter waiting times than the U.S.
I note a couple points about the article linked by Realist. As indicated above, the article suggests lack of funding is the key factor in increased waiting times (i.e. “containment of costs”). Thus, this means that adequate funding could solve that issue. Hence Realist’s objection has little to do with “waiting time” and more to do with not wanting to redirect what we currently spend for medical care from insurance companies to the public sector.
Second, Realist’s linked article provides this interesting information that relates to the “waiting time” argument:
Congress had a Canadian doctor testify recently that wait times are a valid concern? Really?
~ HEADLINE: Toronto doctor smacks down U.S. senators’ myths about Canadian health care.
As Bear points out, the bottom line is that Canadians like theirs and we hate our’s.
https://www.thestar.com/life/health_wellness/2014/03/13/toronto_doctor_smacks_down_us_senators_myths_about_canadian_health_care.html
Porter’s link helps demonstrate another point. These days, probably following Trump’s lead, many folks are no longer willing to state their actual objections to a policy. Instead they make up fake reasons, like the “waiting period” argument, which are already debunked by published objective data, or simply misrepresent what links or stories actually say, apparently in the hope of misleading people who do not check these sources.
I guess they really are uncomforfortable with their actual reasoning – here opposing universal health care coverage simply because they don’t want to see money now spent on insurance and private health care moved to public health care. Maybe it is their stock investments or other dependance on private spending that motivates them, or maybe it is simply the shame of feeling greedy at the cost of care to many in need, but it seems rare to find Trump influenced folks that will admit to their actual motive.
And as noted this comes straight from Trump’s play book – make stuff up, lie about the facts, and project Trumpy weaknesses and misdeeds on others. At least such techniques are now relatively easy to identify and are a fairly reliable basis to summarily reject the arguments of those who use such techniques.
To clarify, the above comment is not directed at Realist personally as only he or she knows his or her personal motive for such arguments.
Likewise, I will acknowledge that there are many people duped by Russian bots and bogus websites who repeat whatever they read with no attempt to confirm it independently so long as it fits their pre-conceived opinions.
As for Realist, he can speak for himself as to his or her personal beliefs and motives since we have never met. I only intend to address the contents of his or her published comments with whatever factual disputes or confirmation of which I am aware.
Appreciate the good discussion here. My main point is that creating more bureaucracy and handing the keys to our healthcare system to the government is a bad idea. Philosophically, I think that is opposite of most people on this forum – hence why I choose to chime in. I dont think adding more agencies, more regulations (to an already overregulated system) would create a better healthcare environment – I think the converse would happen. I would support South Dakota expanding medicaid, which the Noem administration does not want to do. There are alternatives than going to the government for help.
Standard anarchist political troll technique. Inject disinformation into discussions @ issues. Be persistent. Don’t take facts for an answer. Disrupt the discursive process with food fighting. Call it Trumpian – it fits.
Realist – how is replacing the multiple redundant bureaucracies of the private insurance industry with a single point of service “more” bureaucracy. Given the well researched and much proven superior efficiency of operation of the Medicare “bureaucracy” vs the private insurance industry bureaucracies – I would posit the opposite would be the result. Not even going to mention the reduction in clerical work having to be done by doctors offices, hospitals and the like – to only have to interface with ONE payor entity and ONE set of reimbursement rules. Again – that seems to me like it would be a reduction of PRIVATE bureaucracies.
As a reminder – Medicare is currently the single largest provider of health insurance in the US, while also being the most operationally efficient.
Finally – as to the whole “more rules and regulations” thing – are you imagining that the private organizations are rule-free??? Or that THEIR rules may be in conflict with good sense or efficiency?
It seems to me that you want to make some sort of appeal to a “moral” position that government is evil and private business are saints. In fact – neither is true.
I am retired military. My wife and I have MEDICARE and TRICARE For Life as a supplement. We get our meds at the Ellsworth AFB Pharmacy. We can also get our meds by mail thru the TRICARE Pharmacy. My primary care is through the VA. My wife is seen by doctors in the community. All of our “insurance” is a government run program. We pay the monthly MEDICARE Part B premium.
We have experienced several major medical issues over the last couple of years including inpatient in a rehab bed for 60 days and daily physical therapy. My wife had a pacemaker installed. Waiting time for care is the same as being treated in the civilian community. We seldom have a co-pay for care or meds.
A person going to an Urgent Care without insurance must be able to pay for the visit before care is received unless they are suffering from a life threatening or disabling condition. They are referred to the hospital emergency room. The rates are much higher for the ER and the taxpayers wind up paying for the ER visit.
Bring on government run healthcare but subject the contractors running it to close oversight. Give MEDICARE the authority to negotiate drug prices.
Richard makes an excellent point about “government” run programs. The fact is that both private programs and government programs are staffed by human beings, some very capable and honest and some not so much.
Indeed, the motivator to cut corners would seem more likely in the private sector where the individual’s goal is to maximize profit – i.e. get the most money possible from consumers for providing the least service they can get away with.
In stark contrast to private sector employees and investors there is simply no incentive or reward for people employed by the government, or the taxpayers that pay taxes, i.e. invest, in the public sector, to try to make consumers pay more for less.
I will say, however, at least the anti-government reason for opposing all or most government programs strikes me as an honest, if somewhat emotional, basis for opposing medicare for all; much more so than “waiting periods” or “cost of the program” and similar factually debunked objections.
In any event, Richard makes several factually accurate points about the advantage of a public system over a private system. And W R Old Guy’s experiences with the public sector should give every anti-government opponent pause to reconsider his or her fear of the public sector.
Medicare for all will not necessarily lead to lower prices, particularly if the cost drivers are not really addressed. For example, smoking and drinking do not lower the costs of healthcare….and simply imposing medicare for all will not reduce the frequency and volume of either smoking or drinking.
One of the variables not being addressed is the cost of R&D for various drugs….particularly those that require years of research, but then don’t work. The kick in the pants is that you don’t know that they will not work ahead of time. That seems to be a cost of doing business at the moment.
We need the ability to either computationally model the behavior of different drugs well enough to avoid various steps in the current R&D lifecycle (and their expense), or we need to develop different biochemical tests that are more predictive of future behavior.
The lines in Mexico are 100’s deep of Americans buying their meds. Everything from antibiotics to insulin. An elderly couple in line said the states cost them 874$ A month Mexico
$36. Quite a bit of difference.
January thru March is Mexico biggest month for Americans buying their meds.
The manufacturing is unregulated in Mexico, but people trust they r getting the right dose and authentic materials. A worker told me “yes why would we want the reputation of selling fake medications” it’s a million dollar business for their town.
Intaking unregulated products really worked out well for vaping didn’t it?
To pay for safety and reliability, the product will have to cost more. Unfortunately, many are willing to take the chance for the lower cost.
“Intaking unregulated products really worked out well for vaping didn’t it?”
I don’t think the need for life saving meds is analogous to recreational vaping. Nor is it a matter of people “willing to take the chance for the lower cost.”
Real people are actually dying, for a fact, because they cannot afford the meds. A chance at a vial of Mexican insulin beats certain death.
Mac, you blew that one all the way round.
Intaking unregulated products is not good in either case. People are dying in each case.
You missed the mark again.
No, you did and you can’t admit it. Vaping is a choice, an activity. Insulin is a necessity. Without it the body dies. They’re not the same and this is not a game to see who wins.
You casually belittled people who are trying to survive by equating them with vaping teenagers or someone just trying to save a buck. They’re trying to live. Don’t you know that?
Wrong. Whether someone dies due to a bad drug of choice (and the bypassing of safety is completely voluntary), or from not getting the correct and SAFE medicine (particularly for a treatable illness), neither death needs to happen.
I haven’t seen you dodge like this before. It does not enhance your reputation.
T, you failed to mention dental care in Mexico. The best for less. BTW, when is Chubby gonna demand that Obamacare be unconstitutional so he can get rid of it. Make America Grate Again, go back to the days prior to 2010. Chubby is scared to do that as are republicans in general as they know that the main ones receiving benefits from the ACA are folks 65 and older along with White folks (base) in general. The folks that complain the loudest don’t pay for their health insurance, their company does. They don’t realize the actual cost of what they have.
Doc, how much do you pay for your coverage? Realist, how about you, how much a month are you paying and how much is your company paying? Get real.
W R Oldguy speaks the truth. I have also been under VA government care since 1968. No complaints and I’ve had some serious stuff in my life.
Wrong again. I want our healthcare system to solve both problems. Proper solutions will bend the cost curves for healthcare so we can address the other challenges we face.
Hey, how about we invest savings into carbon-free and emission-free energy? That would accelerate the reduction of chronic health issues from particulate matter. Burning coal is in the same category as smoking and drinking….don’t plan on reducing healthcare costs if you do more of any of these.
Deaths from lack of access to insulin, or deaths resulting from the addiction to over-prescribed painkillers, or deaths from the intake of harmful substances in a drug of choice are all deaths. Good holistic healthcare should reduce the deaths in these and other categories.
How much you payin’ doc? That’s a perk you’ve got, nothing wrong with it. In some of those countries listed above, they also have private insurance that sometimes is provided as an extra perk. Of course, that is underwritten so not everyone gets it. But before you begrudge Medicare for All, take a look at how privileged you are from your status. We’re not all equal..like we are aged 65 and older.
Those countries also have a separate Social Security to take care of healthcare, disability, unemployment, family leave, etc. Not a bad deal once you understand that there actually is a lock box on their Social Security. Booyah!
Jerry,
I would agree that the pricing practices in a lot of healthcare are not transparent. It is not really a typical free market. There are some things that are selective or you have some decision time to consider the best care at a lower price. But there are many other things where you need care right now, and/or there is no alternative within your healthcare plan.
Just thought I’d mention that just today I was trying to buy some old standby sulfamethazine for livestock. Not available. Availability of it and several other drugs comes and goes apparently. A new thing. Somehow I don’t think that would be a problem in a really competitive industry.
Years ago I was taking a drug supplied by a generic drug company. Over night the price increased ten fold. I was told by my pharmacist the generic company was bought by one of the biggies and that was the cause of the price increase.
The drug monopolies in this country have run a muck.
I have a slew of relatives in New Zealand and a bunch of friends in Canada. We have pinned them down on their opinions of their healthcare and have never heard a real complaint.
One of my cousins husbands has always worked in healthcare in NZ. For years he has visited patients who have their personal dialysis machines in their home. While we were in NZ he took us to visit one such patient who still was an active owner operator of a sheep “station”. He did his dialysis while he slept. In this country that same patient would have to spend several days a week going to a center for dialysis and because of that could no longer be an active working member of society. New Zealand thinks their way is a safer, cheaper, more humane way of doing things. I agree.
Given that upfront costs and the upper limits for out of pocket expenses are going up, the larger benefit for employer-based health care is the protection it provides against the most expensive healthcare items. The plan does not pay for everything….sorry.
Would you be fine if everyone had the opportunity to join a similar healthcare plan that the members of Congress enjoy? Maybe enjoy is too strong a word, but that could be an option.
Doc, A very good pal of mine got the prostrate cancer. In Colorado Springs, there are two hospitals. My pal could not get treated there for weeks upon weeks because there was no room at the hospital and when there was, the doctor was on a different schedule. His wife was raising all sorts of hell about it, but it didn’t matter, there was no room at the hospital for treatment.
In America, you cannot get immediate care right now unless you go to an emergency room, and you better be bleeding or else there gonna send you home or if you’re bad enough, admit you.
Something else too doc, sometime check out some of these hospitals in South Dakota. Many were built 40, 50, 60 years ago and were built in such a way it’s almost impossible to upgrade them for the needs now. Healthcare needs a total revamp in our ivory tower that would include the trained local workers to man all the stations… without travelers to fill the slots.
The poor bloke that has insurance is paying, or their employer is paying, $1,500.00 a month for the husband, the bride. Add two kids on that plan and you’ve got that easily. Add it all up, that’s if the age is mid 40’s and then it goes up. That total is $18,000.00 a year for a plan that has a $6,000.00 deductible and a family out of pocket of $16,300.00. So that family of 4, about your age, mid 40’s, has an exposure of…let me take my shoes off to add this all up, $34,000.00 each year! So then, how expensive is Medicare for All? Look at the numbers and you will see we pay a whole lot of money for nothing… and we’re still sick as hell because we cannot afford to see a doctor.
Doc, if the health plan that congress has is so good, why did Sean Duffy quit to get Obamacare? “Due to the youngest child’s health complications, including a heart condition, Duffy announced that he was resigning from Congress, effective September 23, 2019, in order to focus his time and attention on his family.”
Regardless of who you are, or what your profession is, American health care is American health scare. If you get sick, they take all your money and your possessions. No where in those countries listed above can you go bankrupt because of medical bills.
McTag sez, “Medicare for all will not necessarily lead to lower prices, particularly if the cost drivers are not really addressed.” Maybe just maybe he’ll explain why the cost drivers wouldn’t be addressed. They’re addressed in my PPO (Kaiser). You can’t smoke and be a member. You can’t be overly obese and be a member. You can’t skip checkups and lab tests and be a member. You can’t do any number of things that drive up Kaiser’s costs and remain a member. I think McTaggart suffers from the continual contrariness so many in SD are infected with, with no known rewards except irritating others to entertain his own boredom.
With regard to hospitals, sometimes you do have to start over. Sometimes you can do a makeover. Sometimes you upgrade where you can. But I would submit that people are a critical part of the infrastructure that is of dire need too.
We should want better doctors to deliver better healthcare, and more of them. Did you know that students with a physics background do better nationally on the MCAT exams than the biology or chemistry or biochemistry majors do? More students with a background in Physics (either a Minor, or a double-major, or a single Physics major with a pre-Med emphasis) would help in my opinion, but I do teach Physics.
One of the treatments for prostate cancer is radiation therapy, and that can also use pharmaceuticals too. So a multidisciplinary background in physics, biology, and chemistry can be very helpful. You cannot do the biomedical engineering either for new treatments and instrumentation without that combo.
Porter just opposes anything I say….Hugs are great.
If you are not reducing smoking and drinking, then you are not reducing a cost driver. If your clean energy plan does not actually reduce carbon nor particulate matter, you are not addressing a cost driver for healthcare.
So Medicare for All would have similar restrictions to your example, and those smoking and drinking in excess would not be eligible for Medicare for All? Interesting.
The assertion that “medicare for all will not necessarily lead to lower prices” misses one goal of public financed health care – reducing the cost as compared to current for profit health care. Cost can’t be assessed in some hypothetical vacuum, rather it must be assessed in relation to a comparative cost – here the cost of providing public health care versus the cost of for profit private health care.
Arguments about the cost of smoking, drinking or other activities that harm health seem nonsensical for such a comparison precisely because there is no basis to conclude that these activities will be reduced or cease to exist in either a private or a public system. A public option could easily do as much, and perhaps more, to encourage healthy habits as any private for profit option.
McTag’s projecting. The problem solving skills involved in physics don’t carry over as problem solving skills when dealing with humanity. The laws of science are rigid, where the abilities of humans are infinitely flexible and capable of adapting. The human brain is the most powerful force in the universe; much more so than the rigid constructs of science. Einstein was genius because he not only knew everything you know Tags but he understood people. There in lies the reason your problem solving skill doesn’t traverse to real world application.
If all the systems and countries listed above are failing, then why is the United States trying to make deals to buy drugs from them for the population here? Why is the United States openly recruiting foreign doctors and trained medical personnel for our healthcare system here?
The drinking and smoking lead directly back to ag producers, that would be hurt even further with a prohibition. If that argument is sustainable, why not penalize farmers for growing the corn that makes corn syrup, milk and cheese that makes Americans develop the fat arse’s. Ranchers provide beef and pork, so let’s close fast food places and restrict what grocers can sell to us on a ration stamp (worked in World War II).
So then, farmers are to blame for the failure of the American healthcare system. So why don’t we give them a way out of this dilemma and allow them to grow hemp. Can’t smoke it and the only way to ingest it would be in liquid form or edible in low grade THC, Make clothes out of it to eliminate cotton. Paper to stop the clear cut of trees that help to cleanse the air. The list goes on. Or we could pay farmers and ranchers as the professionals they are to supply us the products we need to survive.
My neighbor is a nurse in the kidney transplant factory at UW Health. They do the most kidney transplants in the nation. He has some insights into this because many kidney transplants result when people don’t take proper care of themselves, either through diet or taking their medication correctly. Genetics has something to do with kidney problems, as well. Also, kidney diseases can result from uranium and other minerals in the water a person drinks.
He says that a lot of chronic disease that cost money can be reduced, but it requires more in preventive care. This includes good environmental protection and better health education. He thinks really good science and health courses in schools, along with delivery of medical services through schools would be good.
The rate limiting step for kidney transplants is availability of kidneys, which requires the death of a suitable donor. The docs and nurses are ready to go day or night. They have a patient list, so as fast as the patient and the kidney can get to the hospital is how fast the process works. But, the patient list protocol is highly regulated. You have to be damn near dead to move to the top of the list. Economic or racial privilege cannot enter in. Because many of these folks have been sick and with reduced workloads and on dialysis and expensive drugs for years, most have very little money and are on Medicaid or Medicare, which limits how much the docs and hospital can make from the kidney factory.
He said they are not a profit center for UW Hospitals. They break even, most years. For this particular procedure the best way to cut costs is to put money into prevention.
Donald – a factual clarification to your last comment: the availability of kidneys does not require “the death of a suitable donor.” Healthy people can donate one kidney and live out life with little chance of future health problems due to only having one remaining kidney.
https://www.kidney.org/news/kidneyCare/spring10/KidneyDonation
This was one point that I have raised in response to those who seek to deny women the right of privacy over the use of their bodies – If opponents to this right of privacy are honest in stating their goal of saving lives then why don’t they advocate for a mandatory organ donation requirement whereby both men and women are forced to allow someone in need to use their bodies for survival. Indeed, isn’t this exactly the reason that so many, possibly including the new SCOTUS majority, support forcing women to carry and give birth against their will, namely to save another’s life?
Mandatory conscription could apply to all ages, not just women of child-bearing age, for kidney (and even partial liver) transplants and would substantially increase the supply of organs needed for survival. The U.S. could set an example for other countries without a constitutional right of privacy. And after all, sauce for the goose is sauce for the gander.
I disagree with you Porter. Surprise….
Sorry, but the answers to the brand new problems are not found in the back of a book. You cannot memorize your way to a solution for a new problem. Surprisingly, not all problems can be reverse-engineered.
Those problem solving skills from Physics definitely translate. Physics majors make good systems engineers because they understand what the various disciplines are trying to do, and they serve as a bridge between them. The data is clear….students with a Physics background do better on the MCAT.
Medical doctors do need instant recall, familiarity with the biological systems of interest, and knowledge about what has been done before in a similar situation. Physics helps with the process of forming a solution to both integrate those items, and organize a solution to a new challenge. In either case, that process includes working together with other people, including the patient. The physical laws which the body and other diseases must follow also help to constrain the nature of the solution.
And yes, students in physics also take the arts and humanities too.
The two leading causes of kidney disease are diabetes and high blood pressure.
The issue with uranium and kidneys is its chemistry, not its radioactivity. Uranium is a heavy metal. Mercury, cadmium, and arsenic are not great for the kidneys either.
Alas, if there were only a way in which we could remove the uranium from the ecosystem, get a beneficial use from it, while destroying the uranium in the process. It may be that nuclear and renewables have many common recycling needs, and they could work together to solve their recycling problems.
This just in…lithium and cobalt cause kidney damage too. You know, the same lithium and cobalt used in electric car batteries that we are currently throwing away and not recycling? And because we are not recycling, we will need to mine more of each? Good news, the plan is to mine a whole lot of it.
Believe it or not jerry, people are not going to stop smoking or drinking because you and I think it is a good idea. We were making great progress in reducing smoking until vaping came along. But perhaps now with the new age limit we will get back on track.
Bear, Yup, you are right. Kidney donors can be anyone with a proper match. I knew that, too, because one of my friend’s partner got a transplant a few years ago. Thanks for catching and correcting my mistake.
You’re wandering off topic again, Bob. You asserted that the risk factors that affect the cost of healthcare wouldn’t be addressed in Medicare For All. Please, tell us why you can validly declare that. Is it because you have an imbedded bias against government run services, even though you choose to work for a government school instead of a private school? Medicare is widely approved of by those of us who remain healthy because of it. Why demean it with unsupported assumptions?
Yes, let’s stay on topic. Are those conditions you asserted for belonging to a healthcare plan going to be included in Medicare for All? Could you then still call it Medicare for All?
It would make sense that in a Medicare for All that we all do our part to reduce the costs of healthcare. Will those that take on greater risk…by choice…have to pay more in a Medicare for All plan?
Or will the rest of us get to pay for your choice?
In order …
Yes. They will be included in Medicare. My healthcare is paid for by Medicare and it includes those provisions, now.
No. Medicare is Medicare. For all is a qualifier for inclusion.
No. Those that take on greater risk won’t pay higher taxes than those who don’t smoke. Those who take on greater risk will be constantly reminded by their healthcare team to the risk they’re taking on. Not everyone is a contrarian like you, Bob. People listen to their doctors. Especially when they’re sick and don’t want to be.
No. Medicare is for all and paid for by the taxes you pay (at the rate you pay) according to your ability to pay.
Now. I’ve explained it to you. Now, you explain why you think Medicare won’t address risk factors once expanded to all Americans. You started with that assertion. Take the floor and address your declaration.
Medicare has existed for 55 years. It saves money for every one of it’s 60 million participants. Medicare will also save money for every new person allowed to buy a plan. As MFI says, we pay around $180 a month for our Medicare enrollments. On what basis do you, Robert McTaggart, contend that it won’t save money “for all”?
Porter,
With regard to clean energy, you want to go to wind and solar because we have to….but that ignores the reality of the fluctuations in supply and demand that occur, and the other issues with the lifecycle I have brought up.
You are doing the same thing with Medicare for All in my opinion. Ignoring the underlying cost drivers is not the same thing as promoting solutions for reducing them.
In both cases, you are making an argument that we all deserve a better healthcare system, and for that matter we all deserve a world powered by clean energy. That sounds great, who can disagree with either of them. And there is some synergistic effect between the two…more clean energy, less pollution, less strain on the healthcare system.
But declaring that everyone is covered simply doesn’t mean that the system will be better. Covering everybody with a crappy system is not something to crow about.
We need to change how things are done at the same time. For example, we should be working to reduce smoking as much as possible. As I have said before, I don’t see how reducing tobacco smoking but allowing for more marijuana smoking helps in that regard.
Providing coverage for things that should be covered is a winning political argument. Changing the way healthcare is delivered to increase benefits and outcomes to the patient is a winning argument.
I don’t think avoiding taxes but increasing the federal deficit to cover everybody instead is a winning political argument.
“No. Those that take on greater risk won’t pay higher taxes than those who don’t smoke. ” — Porter.
Currently, tobacco smokers do get to check a box and pay more for their healthcare.
Wrong. Smokers on Medicare check no such box. Smokers pay more for supplemental but supplemental is private insurance.
You again assert that, “Changing the way healthcare is delivered to increase benefits and outcomes to the patient is a winning argument.” Duh!
One More Time … Explain why you think Medicare for All won’t do that. We who promote it will demand that. The problem is YOUR negativity not Medicare’s ability to adapt and save money.
~ Big programs are designed and instituted to address big problems. Social Security, Medicare, and Medicaid address old age, healthcare and poverty. They don’t address the hypotheticals continually invented by contrarians, often trying only to irritate others and satiate their own boredom.
Bob, you spend three times as much brain power thinking of why a plan won’t work when you could spend a third as much energy and help make it work.
Contrary is as contrary accomplishes. Very little.
Someone else can address Mr. McTaggart’s newest assertion that Medicare is a “crappy system”. He’s apparently not on board with the beliefs of the majority of Medicare enrollees.
Simply put, proclaiming blanket coverage does nothing to solve the problems of the healthcare system. Keep waving that magic wand…it has to work at some point.
What will a Medicare for All will do to solve the problems? How do you solve the need for more doctors and better doctors?
Also, if you have lower costs that are subsidized by the rest of the population, who will subsidize the costs for the rest of the population when they are covered by Medicare for All?
A wind energy analogy is appropriate here. Wind energy is subsidized because it cannot make money when the wind is not blowing, and there are ongoing costs of business that occur regardless. But if they can reduce the inputs necessary to build the wind turbine, and reduce decommissioning costs and benefit financially from a secondary use of recycled material, then the requisite subsidies can go down. If the energy itself can be delivered without losses or stored for later, then the economics can change.
So reducing the costs of delivering healthcare and avoiding unnecessary healthcare will be important in supporting a “Medicare for All” for a broader population. All I am hearing from you is that the imposition of Medicare will fix everything.
I am so happy to have Medicare. I pay $67 per month for my supplemental insurance.
I have never met a person using Medicare who would rather not have it.
My argument Debbo is really how do you pay for it for everybody, while also dealing with the underlying issues of the healthcare system.
For example, if you do not do something with pharmaceutical costs, those higher costs will just be passed along to us in the form of fees or taxes or added interest rate costs associated with a larger federal deficit. That is how business works. Did you see how the tariffs worked? Higher costs for a business were just passed along to the consumer.
If you want independents and republicans to approve such a plan (and it would not be an honest medicare for ALL without their buy-in) the financial sustainability needs to be clear. We haven’t even solved the long term sustainability for social security yet. That would boost public confidence if that were finally fixed.
Universal health care is so complex and so impossible to pay for that only 32 out of the world’s 33 developed nations have adopted it. And none of them want to give it up for our health care system.
Before I listen to yet another argument about “how are you going to pay for it?” let me know if you asked the same questions about the tax cuts for the wealthy, the war in Afghanistan, and the dramatically increased Pentagon budget. Trillions down rabbit holes and here we are.
Before I listen to yet another argument about wait times, etc., let me know how long it takes to get medical care when you don’t have insurance and there is no local doctor and you literally can’t afford anything.
Before I listen to yet another argument about what about innovation in medicines, etc., if everything’s run by the government, allow me to remind you that NASA invented camera phones, CAT scans, LEDs, athletic shoes, water purification systems, wireless headsets, jaws of life, smoke detectors, artificial limbs, infant formula, and satellite technology, vaccines (hepatitis A & B, flu shots, etc.), etc. And that the government – our taxpayer dollars – already fund most medical research. (See https://other98.com/taxpayers-fund-pharma-research-development/)
There are no real financial, medical, or innovation objections possible to universal health care in this country. The only real objection is that of private health industry – insurance, hospitals, HMOs, etc. – who want to continue to maximize profits and minimize expenses for themselves and their shareholders. A plague on all their houses.
Doc still has not answered the question, “How much do you pay for your health insurance?” Is your health insurance paid for by your boss? Get back to us soon so we can tell you how we pay for Medicare for All, otherwise, you’re just trolling.
Eve nails it!
Republicans had the first two years of the Trump presidency to enact their version of a comprehensive health care plan. They chose to focus on repealing the Affordable Care Act in its entirety or dismantling key provisions of the Act so as to render it functionally useless. They never offered a plan to reduce costs, ensure access, or diminish the possibility that long term care could result in personal bankruptcy.
Contending that Republicans may go along with a comprehensive plan that can be funded in a manner that may have pleased them a few decades ago seems to miss a key point. The party, especially in its current Trumpist iteration, does not consider health care reform or insurance reform a priority.
The ACA may have been flawed. My wife and I have been lucky and always had insurance through our employer, so I never had to deal with the exchanges. Medicare for all may be too expensive. I don’t know. I am certain, however, that congressional Republicans and Trump will not go support or develop any comprehensive plan, paid for or not.
Eve,
Because people have charged the national credit card for trillions for their rabbit holes, we should add trillions to the debt for our rabbit hole. They get a rabbit hole, we get a rabbit hole. That’s how jerry does it….sound financial planning.
If there isn’t a problem about paying for it, then pay for it.
I would express more confidence in a Medicare for All if we had already taken care of Social Security. And we have not done that yet.
I bow down to the wisdom, wit and brilliant sarcasm that is Eve Fisher!
Give it up Mac. You’re the only one who doesn’t recognize that you’ve been pummeled into powder.
Wrong, Mr. McTaggart – there is always a way to pay for the things you want. And I have actually done the math on Medicare for All, and it is perfectly workable, not to mention amazingly affordable. partly – if not chiefly – because (in case you don’t know it) we on Medicare pay premiums! For Part B, Part D, and Supplemental. (BTW – my private health insurance company increased my premiums to almost $1000 a month for my 64th birthday present, knowing I would not dare dump them because I would not be able to get any other private coverage that was any good. Thank GOD for Medicare.)
And we all pay Medicare taxes. You expand the pool, you expand the revenues. As opposed to tax cuts, which shrink revenues to the point where there is mighty little left except, apparently my Social Security and my Medicare, which the GOP Senate is already saying must go to pay for the tax cuts (from my cold dead hands, boys).
Another reason for affordability is that once everyone actually gets health care, costs go down because they get free vaccinations, maintenance health check-ups, etc., and they’re finally not running to the emergency room with every ailment because they can’t afford a doctor, nor are they waiting to see the doctor until they are, literally, dying.
Meanwhile, continue to come up with every excuse you want as to why universal health care is unaffordable, etc., but you’re barking in the wind, my friend, barking in the wind. It is affordable, it is humane, it is the only way to rein in skyrocketing health costs, but you just don’t want it. So I am done talking to you. Goodbye.
POWDER!! BARKING IN THE WIND!!
Doc wants us to go down the rabbit hole because he knows the answer to the question put in front of him. Damn..If I answer it, everyone will know I’m a troll. Guess what doc, we already know. As easy to read as Beetle Bailey.
Yet another screwing by drug company’s for 2020.
“Drugmakers including Bristol-Myers Squibb Co, Gilead Sciences Inc, and Biogen Inc hiked United States list prices on more than 50 drugs on Wednesday, but they are not the only companies demanding that consumers pay more. The prices of more than 250 drugs increased in price this New Years’ Day, according to data analysed by healthcare research firm 3 Axis Advisors.
Reuters reported on Tuesday that drugmakers including Pfizer Inc, GlaxoSmithKline Plc and Sanofi SA were planning to increase prices on more than 200 drugs in the US on January 1, 2020.” Look to the north of us or to the south of us where you can buy all the drugs you want for less than a quarter of what you pay here. Plus, ya got good fishing to the north and plenty of sun to the south. The only draw back is the violence that you will miss by going in either one of those places.
One of the issues we have discussed often that shortens life is the opioid abuse epidemic. Large studies seem to return to two causes.
1. Loss of job. The blue collar work of coal mines, auto plants and such are especially highlighted examples.
2. Accessibility of the opioid.
Even in areas where jobs were nose diving, if Big Pharma was not pushing the painkillers, addiction was lower. Both items appear to be necessary to kill people. “Deaths of despair” via opioid addiction necessarily include easy access to the med to initiate the addiction, which is often replaced by heroin.
Big Pharma CEOs belong in prison.
The Atlantic
is.gd/7DdpDJ
States that added the Medicaid program saw a 6% reduction in opioid overdoses. That’s from JAMA.
One week to build a new 269,000 square foot 1,000 bed hospital! Amazing. And then they rested.
“The Chinese city of Wuhan is set to build a hospital in six days in order to treat patients suspected of contracting the coronavirus.
There are currently 830 confirmed cases in China, 41 of whom have died.
The outbreak began in Wuhan, home to around 11 million people. Hospitals in the city have been flooded with concerned residents and pharmacies are running out of medicine.
According to state media, the new hospital will contain about 1,000 beds.
Video footage posted online by Chinese state media shows diggers already at the site, which has an area of 25,000 square metres (269,000 square feet).
It is based on a similar hospital set up in Beijing to help tackle the Sars virus in 2003.
“It’s basically a quarantined hospital where they send people with infectious diseases so it has the safety and protective gear in place,” said Joan Kaufman, lecturer in global health and social medicine at Harvard Medical School.”
Can you imagine that being done here? Me either. Take us that long to find a shovel.
26 states now treating symptoms of coronavirus, so it’s coming. Bet we wish we would’ve expanded Medicaid, but no way here man, we’re on our owm.
Jerry … I put photos of the hospital China built, on Twitter and got a lot of comments on Communist forced labor and Muslim internment camps. China has been over-villainized for political benefit and comparisons to ImPotus’ tyranny, I suppose. Wishing the populist movement would run its course.
Good god Porter do you ever listen to yourself. China is detaining its own Muslim citizens, not far from torture trying to force them to give up their religious practices, but we’re over-villainizing them? In the next sentence you vilify this country for simply wanting to restrict immigration of those with the same religion. We’re horrible but they’re over-villainized. Unbelievable.
“Residents said people have been sent to the camps for visiting relatives abroad; for possessing books about religion and Uighur culture; and even for wearing a T-shirt with a Muslim crescent. Women are sometimes detained because of transgressions by their husbands or sons.”
https://www.nytimes.com/2018/09/08/world/asia/china-uighur-muslim-detention-camp.html
I tend to believe, Porter, that China could achieve a good end without its brutal approach to dissidence.
Gosh, Contrary Camper. I so wanted you to be my pal, too. Cold up there, isn’t it? Low 50’s here, this week.
In the meantime, South Dakota has no Medicaid Expansion to take care of those of us who cannot afford to be taken care of until they are so sick they come to the emergency rooms.
Other, civilized nations, have healthcare in place that will rise to make sure all of the populace is as protected as possible, and are taking steps now. Meanwhile, here in the land that doesn’t give a crap, we are screwed. Do you go to see the doctor and trigger a $16,000.00 dollar out of pocket, or do you just hope that you don’t die alone? Rapture my arse.
I read about China’s instant hospital and I’m both flabbered and gasted. In a week?! The concrete won’t be cured! Still, when you’ve got a few Billion people and a highly contagious disease breaks out, I guess a little panic is in order. Wow.
It would be nice to see some pro-health panic break out in the USA among the GOP. I wonder how many coronavirus deaths would be required for them to notice? Apparently the opioid addiction deaths haven’t been enough. Increased maternal mortality is insufficiently deadly. Increased suicides? Gun deaths? What is the magic number of dead Americans for the GOP to care? Is there a number?
Debbo, the answer to the question “Is there a number?” is “No.”
Whatever it is, unless it actually impacts the Republican individual, in Congress, and elsewhere, it is irrelevant and – as one memorably told me about a true story from my childhood – “anecdotal”, which makes it even more irrelevant.